Nigeria State Level Public Health Emergency Operations Centers Case Study
Jan 7, 2021
James Banaski1&, Winifred Ukponu2&, Everistus Aniaku3, Andebutop Ashasim Elisha4, Charity Ezeudu5, Stephen Fagbemi6, Ibrahim B. Gobir2, Kamaldeer Khadeejah7, Piring’ar Mercy Niyang2, Peace Nwogwugwu8, Ryan Remmel1,9, Rabi Usman10, Claire J. Standley1‡
1 Center for Global Health Science and Security, Georgetown University, Washington, DC, USA
2 Georgetown Global Health Nigeria, Georgetown University, Ajuba, Nigeria
3 Directorate of Emergency Preparedness and Response, Nigeria Centre for Disease Control, Abuja, Nigeria 4 Office of the Director General, Nigeria Centre for Disease Control, Abuja, Nigeria
5 Public Health Emergency Operations Center, State Ministry of Health, Enugu, Nigeria
6 Public Health Emergency Operations Center, State Ministry of Health, Ondo, Nigeria
7 Public Health Emergency Operations Center, State Ministry of Health, Kwara, Nigeria
8 Public Health Emergency Operations Center, State Ministry of Health, Abia, Nigeria
9 Walsh School of Foreign Service, Georgetown University, Washington, DC, USA
10 Public Health Emergency Operations Center, State Ministry of Health, Zamfara, Nigeria
&Equal contribution
‡Correspondence to Claire.standley@georgetown.edu
Key Facts
- Nigeria has developed a national Public Health Emergency Operations Center (PHEOC), called the National Incident Coordination Centre (NICC), as part of the Nigeria Centre for Disease Control (NCDC) and is assisting in the development of PHEOCs at the State level. As of December 2020 all the 36 States and the FCT do have functional Public Health Emergency Operations Centres. A few of these PHEOCs are yet to have permanent workspaces, but coordination along the Incident Management System does occur.
- State PHEOCs have received development assistance from the Nigeria Centre for Disease Control in the form of needs assessments, planning documents, training materials, etc.
- The NCDC NICC was activated to support the COVID-19 response, and plays a central coordination role in collecting, analyzing, and disseminating data, as well as operational and logistical functions, and provision of support to State PHEOCs, which were also activated in support of the COVID-19 response.
- The COVID-19 pandemic has stretched the capacity of PHEOCs in terms of systems and staff, reducing implementation of other essential health services.
- At the initial stages, PHEOCs faced challenges such as inability to meet regularly and document such meetings appropriately. Many of these challenges where due to inadequate capacity for coordination, but this has markedly improved with the visibility which the COVID-19 pandemic has given to the PHEOCs with increasing support from NCDC and Partners.
- Resource mobilization, physical structure renovations, staffing, surveillance activities, and technical expertise in emergency management were all identified as areas needing to be further developed as a result of operations during the COVID-19 response. A recent PHEOC Assessment conducted nationwide revealed varying levels capacity in terms of staffing, infrastructure and process across the PHEOCs ranging from those which were rudimentary to very developed PHEOCs.
- PHEOC personnel would benefit from the availability of self-directed training resources, particularly in modular formats, as well as targeted in-person technical assistance in areas such as simulation exercises and reviewing SOPs.
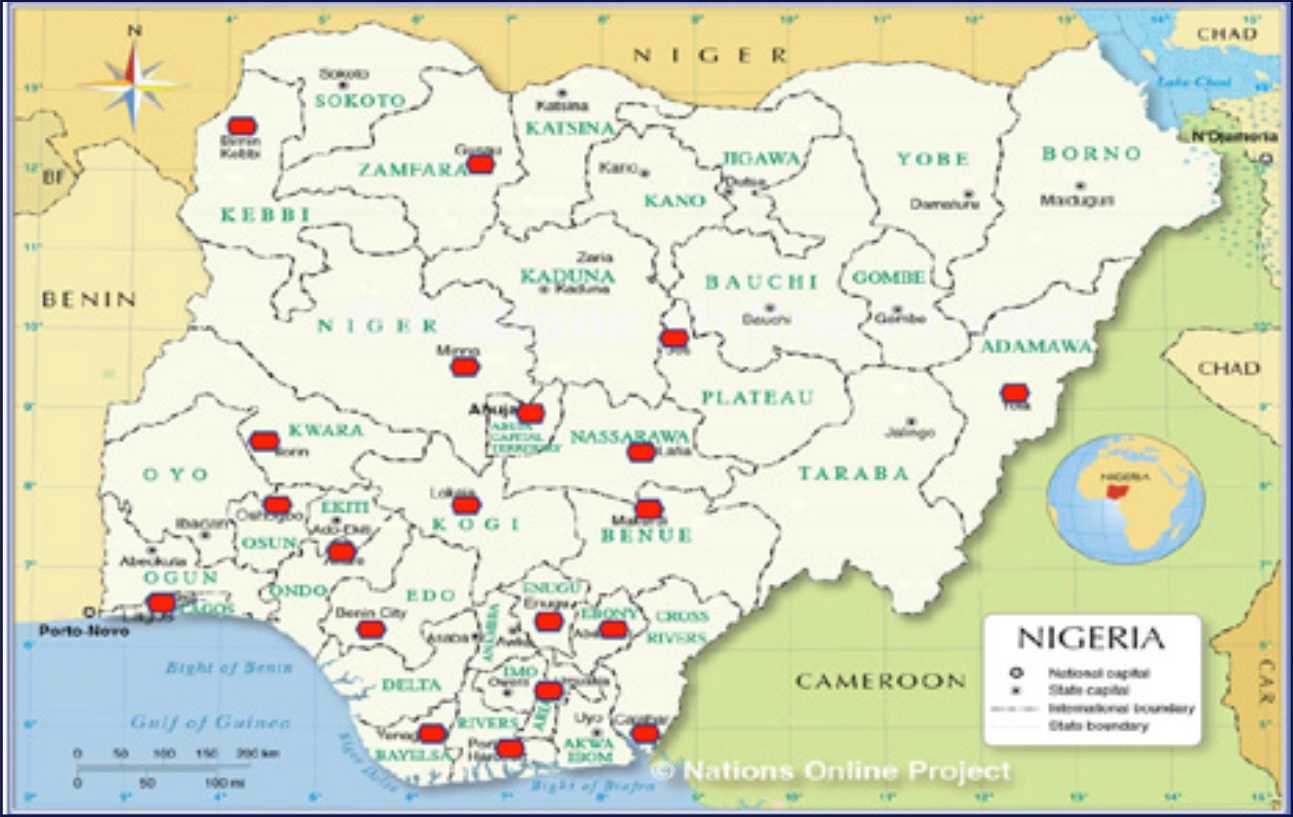
Map of State level PHEOCs in Nigeria. Adapted from the Administrative Map of Nigeria from Nationsonline.org.1
Establishment of PHEOCs at the National and State levels
The Federal Republic of Nigeria, through the Nigeria Centre for Disease Control, developed the National Incident Coordination Center (NICC) in 2017. The NICC serves as the PHEOC during an outbreak or other emergency requiring support from the Federal Ministry of Health. The NICC monitors outbreaks and public health events 24 hours a day/7 days a week, serves as the PHEOC during an emergency, manages the deployment of Rapid Response Teams (RRTs), serves as a central networking location for State level PHEOCs, and is staffed by trained professionals that can deploy within two hours or less.2
As part of the development of the Public Health Emergency Management (PHEM) program at the NCDC, the Head of the NCDC’s Health Emergency Preparedness and Response Department trained with the US Centers for Disease Control and Prevention (US CDC) for four months as part of the PHEM Fellowship. The fellowship teaches how to manage and operate a PHEM program, which is usually where the PHEOC sits within an organization. The fellowship graduates return to their countries equipped to develop, operate, and maintain a PHEM program, which can include developing similar programs at the State, or sub-national level.
As part of that PHEM program, the NCDC assists States in developing their own PHEOCs within the State Ministries of Health. In this vein, NCDC has provided technical assistance in the form of documents and templates, supply chain support, training sessions
on topics such as Incident Management, as well as participation in simulation exercises. While development has been going at a steady pace, not all States within Nigeria have a fully equipped spaces for the PHEOCs, although NCDC has provided basic ICT and other office equipment to all state PHEOCs since the beginning of the COVID-19 pandemic. As of 12 October, 2019, there are State level PHEOCs in 20 states: Zamfara, Cross-River, Enugu, Ebonyi, Bayelsa, Lagos, Ondo, Edo, Nasarawa, Kogi, Kebbi, Plateau, Rivers, Anambra, Niger, Benue, Osun, Kwara and Abia states and the Federal Capital Territory (FCT), however rapid progress was made in 2020 due to the need to effectively coordinate the COVID-19 response with all States now having a functional PHEOC.1 Efforts are ongoing by NCDC to optimise these PHEOCs to make them fit-for-purpose and to all fit in effectively into a national network of PHEOCs. In some cases, international partners have also supported the development and maintenance of State Ministry of Health PHEOCs. The World Health Organization (WHO), the African Field Epidemiology Network (AFENET), the US Centers for Disease Control and Prevention, the Red Cross, the United Nations Children’s Fund (UNICEF), Georgetown University and United States Agency for International Development (USAID) amongst others, have all provided support for the development of PHEOCs at the State level. These outside organizations have provided funding, training, documents, technical assistance, and guidelines on how to establish, operate, and maintain a PHEOC.
Supporting the COVID-19 Response in Nigeria
When COVID-19 began affecting countries around the world in January 2020, the NICC began preparations, including sharing case definitions with health workers, distributing information on personal hygiene and other transmission prevention measures, and readying activation of the incident management system.3 On 27 February, Nigeria confirmed its first case of COVID-19, in an Italian citizen working in Lagos State who had recently returned from Milan, and the NICC was activated. Nigeria was the first country in sub-Saharan Africa to confirm a positive COVID-19 case. As part of the network of PHEOCs within Nigeria, the State level PHEOCs subsequently also activated. The response in Nigeria was established as a Presidential Task Force, using an Incident Management System, to provide technical coordination from the National level to the State level PHEOCs. The NICC coordinates with multi-sectoral partners such as the Federal Ministry of Health, Federal Ministry of Agriculture and Natural Resources, the Federal Ministry of Commerce and Tourism, the Federal Ministry of Defense, and the Ministry of Foreign Affairs, to provide health related direction and coordination during the pandemic. At the State level, the State Ministry of Health’s PHEOC does the same thing, providing multi-sectoral coordination and response leadership.
State Ministry of Health PHEOCs serve as a focal point at the State level for coordination of the COVID-19 response and are responsible for the data that are collected during the response, such as epidemiological data, surveillance data, case management data, laboratory data, as well as data from partners, such as data about personnel entering the country through ports of entry (PoEs) such as land border crossings, airports, and sea ports. The PHEOC also serves as a central location for the dissemination of communications information to the State focusing on messaging to the public within the State.
State level PHEOCs have limited resources, including of money and personnel. Early on in the response to COVID-19, several States have had to either shut down, or temporarily suspend, other response operations or day-to-day programmatic work such as immunization campaigns, nutrition programs, neglected tropical disease programs, and tuberculosis programs. Surveillance programs such as measles and acute febrile illness (AFI) have been greatly affected due to the diversion of resources to support COVID-19 surveillance activities in some States. In other States, it has been reported that the shift to support COVID-19 has not affected any other response operations or day-to-day programmatic work. The situation is gradually improving with all services being provided, and the health system gradually adjusting to the ‘new normal’ of providing all routine services despite the pandemic, although the pandemic has further strained an already stretched health system even pre-COVID-19 pandemic.
Another issue identified during the COVID-19 response at the State level was the reliance upon face-to-face meetings and response operations. While some response operations cannot be done virtually, such as testing operations, certain response operations can and are being done virtually. Unfortunately, most States were not prepared to operate in a virtual environment. The current plans for how to operate in a PHEOC did not contain information on how to run a response in a virtual environment, so the States were slowed down by finding low cost, low bandwidth solutions for conducting briefing and planning meetings virtually.
The COVID-19 response has shown some States that are in further need of development in the area of PHEOCs. The response to COVID-19 has exposed the lack of resources, such as personnel, money, and facilities. Specifically, the areas of resource mobilization (the process of getting resources from the provider and applying those resources to a response), structural renovations (providing a better physical structure for the operation of a PHEOC, technical expertise (training of personnel in topics such as Incident Management, resource allocation, and public health technical topics such as epidemiology, risk communications, and risk management), as well as support to the local levels.
Applying Lessons Learned and Continued Development
There have been many lessons learned from the COVID-19 response so far, such as the need to better mobile resources, development of a cadre of trained personnel to support response operations, and developing plans, policies, and procedures for working in a virtual environment. The PHEOC assessments at the State level served as reflective guides on the status of operationalization, and would be useful to conduct periodically. The State Ministry of Health PHEOCs have also identified the need to further adapt tools from the NCDC, as well as tools provided by outside organizations such as WHO, US CDC, UNICEF, and others. The development of a Nigerian National Framework for PHEOCs could be one way to provide a clear and comprehensive system for operations, training, and future capacity strengthening.
While in-person training has been the preferred method for many years in delivering targeted technical assistance, the COVID-19 response has shown that meeting in person sometimes is not safe or possible in some instances. The shutdown of global and domestic travel due to the pandemic has shown the need for a different delivery method for technical assistance. State PHEOC points of contact have identified the need for self-directed, online learning opportunities as a helpful step in furthering the development of PHEOCs at the state level. It has been acknowledged that access to these materials alone will not be sufficient, but they serve as a starting point for education about PHEOC operations and management, as well as a source of materials to be used in training staff both at the State level as well as the local level.
For example, it has been identified that the States would like more involvement in simula- tion exercises to ensure plans, policies, and procedures are as good as they can be prior to an emergency. States postulate that using an online platform to “teach” the basics of simulation exercise doctrine and how to develop and execute an exercise, as well as how to evaluate an exercise, can be followed up with targeted technical assistance (delivered virtually if needed). This may help set the State up to be able to develop, execute, and evaluate their own simulation exercises, thus reducing the reliance upon outside organi- zations to provide that service for them.
Staff for PHEOCs at the State level agreed that having a PHEOC in the time of an emer- gency is extremely helpful and can help save lives. The challenge most of them continue to experience is the lack of resources (money, facilities, and staff), as well as the need for further training and exercise support. Despite the obvious challenges posed by the COVID-19 pandemic, it has brought some advantages such as giving high visibility to the State PHEOCs especially with the political leaders and other policy makers. Public health professionals must find a way to maintain this visibility and place PHEOCs optimisation on the agenda of relevant policy makers at all levels, to ensure strengthening of health security at the subnational levels especially to complement the relatively well developed capacities at the national level, without which there can be no hope of achieving health security in the country.
Endnotes
- Administrative map of Nigeria, 3 November 2020, https://www.nationsonline.org/oneworld/map/nigeria-administrative-map.htm
- Nigeria Centre for Disease Control, Protecting the Health of Nigerians, 3 November 2020, https://ianphi.org/\_includes/documents/sections/tools-resources/annual-meetings/2019annualmeeting/ncdc-progress.pdf
- Adepoju, P. Nigeria responds to COVID-19; first case detected in sub-Saharan Africa. Nature Medicine. https://www.nature.com/articles/d41591-020-00004-2